Leading Medical Records Retrieval Solution with a Risk-Free Consultation!
Schedule a brief, no risk consultation to learn why ChartRequest is the #1 medical records retrieval and release of information software and services solution.
Schedule a Personalized Consultation
Contact Our Support Team
ChartRequest is Proudly Partnered With
Secure
SOC 2 and ISO-270001 Compliant With Military-Grade Encryption and Security
HIPAA Compliant
Regularly Audited to Ensure Compliance With All HIPAA Rules
Top-Rated
Our White-Glove Service Makes Us the Top-Rated ROI Vendor on Google
Get Records You Need When You Need Them
ChartRequest makes medical, imaging, and billing records more accessible than ever for patients and professionals.
Healthcare Providers
Our release of information solution is purpose-built to streamline the exchange of PHI, reduce status update phone calls, access powerful reports, and so much more. Keep the process in-house, or let our experts release records for you.
This can help your practice:
Support referral management and care coordination,
Prevent Right of Access and information blocking issues,
Minimize the risk of human error with an easy-to-use workflow.
Lawyers and Attorneys
Tired of constantly calling for status updates when you need a client’s medical records? Automate the follow-up and easily beat court deadlines by letting our experts chase records for you with CaseBinder.
CaseBinder helps lawyers and attorneys:
Submit record requests quickly on our easy-to-use platform,
Access status updates 24/7 while our team works on retrieval,
Save on retrieval costs for every request we process.
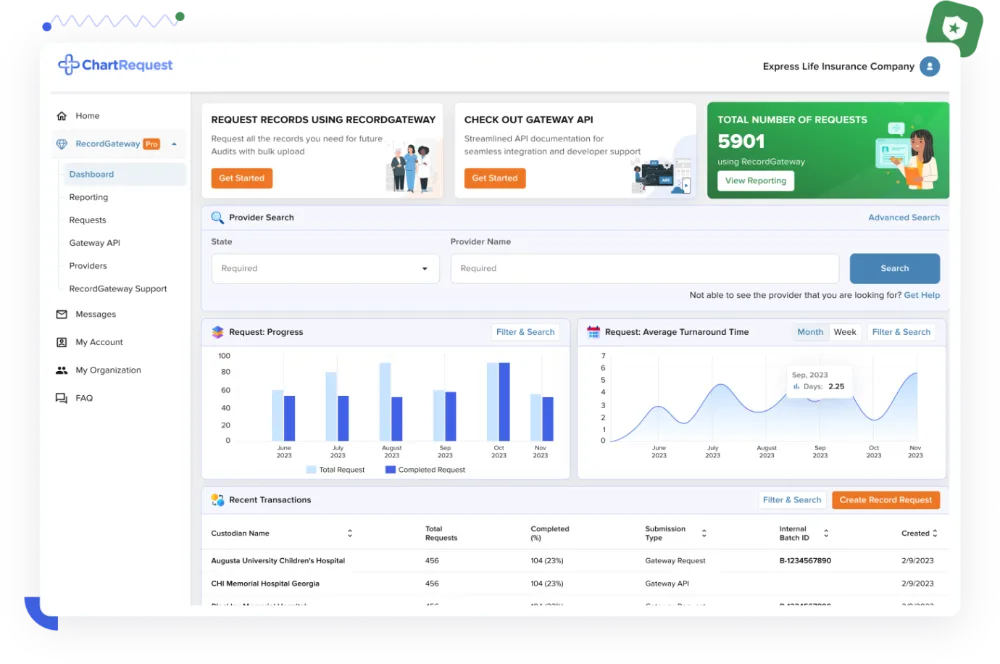
Insurance Companies
During audit season, your insurance company can’t be kept waiting on medical records. Trust the retrieval experts with over a decade of experience to get the records you need quickly and efficiently.
RecordGateway simplifies record retrieval for payors by:
Access real-time status updates to monitor progress for large requests,
Get records with uniform naming conventions that fit your needs,
Maximize retrieval customization with our RecordGateway API.
Patients and Families
Build your personal health record, and rest assured knowing your and your family’s medical information is safe and available to share with your healthcare providers.
ChartRequest Store & Share empowers patients with:
Schedule a Personalized Consultation for Our Medical Record Exchange Solutions
ChartRequest helps patients and professionals simplify the release and retrieval of medical, imaging, and billing records by providing purpose-built solutions and white-glove service.
Benefits of Working With ChartRequest Include:
One-Stop Shop For Records From Any U.S. Provider
Industry-Leading Speed and Follow-Up Protocols
Centralized Dashboard to Organize Your Requests
Real-Time Status Updates and Comprehensive Reports